Overview
This Costing Concept explains how the Parliamentary Budget Office (PBO) estimates changes in bulk billing behaviour in response to policies that affect the Medicare Benefits Schedule (MBS) and Bulk Billing Incentives (BBIs).
The approach is used to support the estimation of financial implications for policy costings. It does not predict clinical behaviour or model patient health outcomes. The PBO regularly reviews and updated our assumptions when new evidence comes to light, which may not be reflected in this Costing Concept.
Bulk billing in Australia
Outside of the hospital system, medical services are generally private businesses with practitioners setting their own prices to cover their salary and other expenses.
The MBS subsidises eligible medical services, reducing out-of-pocket fees for eligible patients. It consists of ‘MBS items’ for which there is an associated ‘MBS benefit’ amount that a patient claiming that service would receive, as set by the Australian government.
- If the practitioner accepts the MBS benefit as the full payment, the service is bulk billed and the patient has zero out-of-pocket fees.
- Alternatively, the practitioner may charge the patient an out-of-pocket fee in addition to receiving the MBS benefit.
Example: MBS benefits, bulk billing and out-of-pocket costs
For example, a practitioner charges $50 to provide a given service:
- If the MBS benefit is $40, the patient may be charged a $10 out-of-pocket fee to make up the difference.
- If the MBS benefit increases to $50 and the practitioner’s price remains the same, the practitioner may choose to bulk bill the service (that is, charge $0).
In this system, the government provides a fixed subsidy and practitioners set their own prices.
Bulk billing incentives
Bulk billing incentives (BBIs) are additional payments to encourage practitioners to bulk bill.
Currently there are 2 types of BBIs:
- Patient level incentives - can be claimed if a given patient is bulk billed.
- Practice level incentives - can be claimed if every patient is bulk billed at that practice.
Unlike MBS benefits, these are ‘all or nothing’ incentives such that a practitioner can only claim these BBIs if they bulk bill the patient, that is, there is no out-of-pocket fee.
Example: MBS benefits, BBI and out-of-pocket costs
For a service that has an MBS benefit of $40:
- If a practitioner charges $50 to deliver the service and receives a $40 MBS benefit plus a $10 BBI, they can break even by bulk billing.
- If the price to provide that service increases from $50 to $55, bulk billing will result in the practitioner falling short by $5. In this case, the practitioner may choose to either accept the loss or charge the patient and lose access to the BBI. If they do charge the patient, the practitioner would need to charge $15 to cover the price rather than just the additional $5 due to the loss of the BBI.
Estimating practitioner billing behaviour
To estimate the financial implications to increases in the MBS benefit and/or the BBI, the PBO divides services into 3 groups:
- Already bulk billed services
‒ Services that would have been bulk billed anyway without the policy change.
‒ Costs reflect any change in the MBS benefit or BBI for the bulk billed services. - Newly bulk-billed services
‒ Services that would have had an out-of-pocket fee to the patient but would become bulk billed under the policy change.
‒ Costs reflect any change in the MBS benefit of the services as well as the additional BBI for the new bulk billed services. - Services that remain patient charged
‒ Services that retain an out-of-pocket fee for the patient regardless of the policy, that is, these practitioners would not change their billing behaviour.
‒ Costs reflect any change in the MBS benefit of the services only. There will be no impact on BBIs as these services are not eligible.
Estimating billing behaviour
In reality, billing behaviour is complex and practitioners juggle a number of factors when deciding what to bill their patients. For costing purposes, the PBO applies a simplified and consistent approach.
The core assumption is that practitioners will seek to maximise revenue in response to policy changes and will switch to (or away from) bulk billing where it is financially competitive compared to charging out-of-pocket fees to patients. This is applied at the practice level or small geographic areas using the latest billing data.
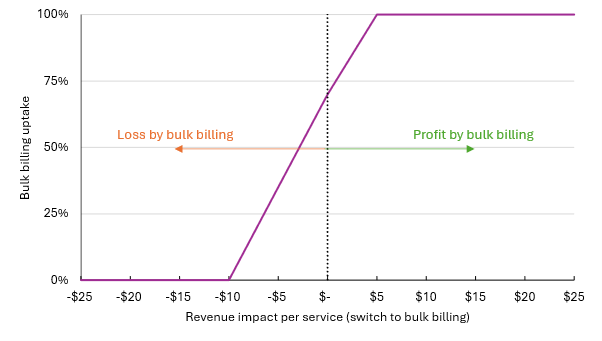
To accommodate non-financial factors, PBO applies an adjustment to preference bulk billing adoption when revenue is equal to, or slightly below, estimated revenue with out-of-pocket fees charged to patients. This is a linear scale based on the estimated per service revenue differences at which practitioners would switch, as shown in Figure 1 below.
- No practitioner is assumed to bulk bill if it would reduce revenue by more than $10 per service.
- Uptake would grow to 100% where bulk billing remuneration is $5 higher than patient fees (this is, where practitioners would on average make $5 more by bulk billing than continuing to charge patients). This upper ceiling is to capture differences in business costs between practices in an area.
Figure 1: PBO assumed bulk billing uptake curve